Would you like fries with that?
The McDonaldization of Psychotherapy: More treatment manuals, more diagnoses, longer and more expensive training, and more therapy speak...and mental health outcomes are not improving. What gives?

As I prepare for another year of teaching social work theory and practice and counseling subjects, I was reflecting with my teaching team on which areas of our subjects we could strengthen. This led to more reflection on the medical model and decision-makers' tendency to lean towards manualized treatments and to medicalize human distress.
Here are some words on the topic.
The McDonaldization of Therapy
McDonaldization is a term coined by sociologist George Ritzer to describe the process where the principles of the fast-food restaurant industry, like efficiency, calculability, predictability, and control, are increasingly dominating more and more sectors of society globally, extending beyond food service to education, healthcare, and therapy, among others. Related to my work, it’s been applied to outdoor education for a few decades. Let’s apply it to therapy.

At the heart of the medical model is a deceptively simple idea: psychological distress is a disease, much like diabetes or hypertension. Therefore, effective treatment must diagnose it before we administer the empirically supported treatment. One simple solution is to medicate. That way, we know the accurate dosage and how the chemical intervention will impact the chemical imbalance scientists claimed to exist but never found.
Manualized therapies follow a similar logic—distill human suffering into standardized protocols that can be measured, replicated, and billed. This approach makes institutions, like insurance companies and other third-party payers, feel comfortable. However, many people who could benefit from effective care still fall through the cracks and disengage from the “treatment.”
But who cares? No one is paying for outcomes. They are paying for the process (diagnosis and manual). Whether it works or engages the help-seeker? Meh.
Regarding McDonald's, we know a Big Mac is supposed to taste the same in Anchorage or Tallahassee. Similarly, manualized cognitive-behavioral therapy is supposed to look the same whether it’s a thought record in New York or Texas.
I often wonder what Freud, Jung, William James, and Jane Addams (among many others) would think about how psychotherapy has evolved. “Would you want fries with that?” Freud might ask.

The Big Mac should taste and look the same no matter who the provider is, their qualifications, years of practice experience, or any other factors we tend to stress. On paper, this looks clean and reassuring. It provides us with a sense of clinical safety. If we follow the manual, then I’ll be effective. If I get the right training, then I’ll be effective. With the right supervision, I’ll be effective.
In practice, lots of this might make sense. But while promoting Kids These Days on various therapy-related podcasts, many tell me they feel boxed in. Many therapists say something along the lines of “I know I’m supposed to follow the manual, but I just do [Insert another modality].” We wrote in Kids These Days that 90% of surveyed psychologists admit having ethical concerns about psychiatry’s bible: the DSM. Is there anything we can do about it?
In January, the American Psychiatric Association shared a roadmap to a new DSM. The S in DSM will now stand for scientific, and they claim to be taking a closer look at biomarkers they’ve historically never found, while simultaneously embracing context. According to Dr. James Davies, “the Chair of DSM-6 (future directions panel) has received unrestricted grants &/or lecture fees from AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Jansen, Otsuka, Pfizer, Sanofi-Aventis & Shire. Her family owns stock in Bristol-Myers Squibb…”
So it looks like the medicalization of distress is here to stay.
If You Follow the Manual, You Have Permission to Blame the Client
When Prochaska and DiClemente developed their transtheoretical model of behavior change in the 70s-80s, unintended outcomes began to emerge in my training. I don’t believe this was their intention, but I’d be interested to hear what others think.
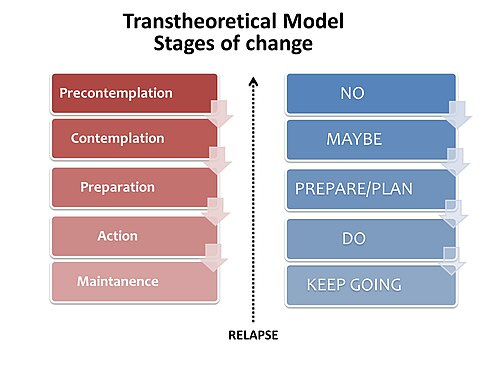
A “stage” is a place in time. A thumb tack placed on a non-linear timeline as to what someone is experiencing on their change journey. But all of a sudden, and we’ll hear it a lot, it becomes a way to describe your client.
Therapy Example
“Why did the client not return to therapy?”
"They are precontemplative.”
“Ah, I see. Did you follow the treatment manual?”
“Yes. Perfect administration.”
Gross Dating Example
”Why did that person throw that drink in your face?”
”They wanted to talk, but I suggested we go somewhere else.”
”Did you say anything rude or off-putting?”
”No. They’re just precontemplative to dating me.”
”Ah, no problem then.”
The therapist isn’t to blame. If someone is feeling precontemplative, the therapist should ditch the manual. They should listen, empathize, remain nonjudgmental, provide information that may interest the client, and use harm-reduction strategies. They should not move the therapy faster than the client and should definitely not start prescribing goals based on what they think is more important than the client. But this is the risk of medicalizing and manualizing human distress.
Human Distress Does Not Occur in a Vacuum
Trauma, poverty, family systems, school systems, grief, and meaninglessness do not show up neatly as “disorders,” yet the medical model insists we force people’s distress into diagnostic boxes anyway. One critique (and serious warning sign) I have about Jonathon Haidt’s The Anxious Generation is that it would be much easier to let everyone keep their phones if we just gave everybody Xanax. We have pills for anxiety, and labelling and medicalizing the entire generation is reckless. I wrote last year that mandatory mental health screening, as Illinois has written into law, has one sure-fire result: rates of mental illness will continue to rise.
When we reduce people to symptom clusters, we subtly tell them there is something wrong with them, rather than responding to abnormal conditions normally. Manualized therapies fare no better once we leave the laboratory. While structured approaches like CBT can be helpful for some, claims of superiority largely disappear in real-world settings. Meta-analyses have consistently found no meaningful advantage over non-manualized therapies, and dropout rates regularly approach 50%. Clients don’t leave because they “resist treatment.” More often than not, clients disengage because of something wrong in the therapeutic alliance, which consists of 1) a relational bond, 2) agreement on the goals or purpose of the therapy, and 3) consensus as to how the therapist and client are going to work together.
No client has ever left my office and said, “Hey, Mom, thanks for bringing me to see Dr. Will. I don’t think he can help and he’s an idiot, but hey, at least he’s evidence-based and trauma-informed!”
That joke I owe to my mentor, Dr. Scott D. Miller.
Follow the Money
So why does this system persist? Follow the money and the power. Insurance companies require diagnoses to justify reimbursement. Universities fund biomedical research because it looks rigorous and profitable. Professional organizations, often entangled with pharmaceutical interests, keep reinforcing the same story, even as the evidence collapses under scrutiny. We still have no reliable biomarkers for most psychiatric diagnoses, enormous heterogeneity within categories, and disappointing long-term outcomes.
Yet the machine rolls on.
What gets lost in the process is the therapeutic relationship—the single most robust predictor of engagement change. Decades of research show that alliance, trust, and attunement matter more than technique. But manuals don’t train presence. They train compliance.
There is actually data showing that, even though therapy outcomes have not improved since our first meta-analysis in 1977, new graduates’ outcomes in the US are starting to decline. We are training people to administer the manual…to craft the perfect Big Mac. Not the interpersonal and dynamic responsiveness required to work with a range of people.
If we want a more humane mental health system, therapists can start by loosening their grip on rigid protocols and listening more closely to the person in front of them. Distress makes sense when placed in context. Growth matters as much as symptom reduction. And therapists need space to think, feel, and respond creatively rather than follow scripts.
Mental health care doesn’t need more manuals or treatments. We need thought leaders and policymakers with the guts, courage, curiosity, and a willingness to let us treat people like people.
I think you would really enjoy reading retired professor of Social Worker William M Epstein’s books - try these
The Illusion of Psychotherapy
Psychotherapy as Religion
Psychotherapy and the Social Clinic in the United States, soothing fictions.
He’s written others.
Love this! Taylor swift instead of an indie artist, Starbucks instead of a speciality roaster, KFC instead of a Michelin 3-star restaurant. I think therapists are great at translating what they’re actually doing into the language of manualized treatment, just like 30 years after a rock band goes platinum there’s a Netflix documentary deconstructing their process of writing songs.